


How Many Covid Deaths Would Ivermectin Have Saved?
The evidence is highly conflicting but it appears hundreds of thousands might have been saved


Tens of millions of people worldwide have listened to the Joe Rogan Experience podcast with Dr. Robert Malone, where the good doctor, who played a vital role in the development of mRNA vaccines, makes numerous controversial claims, including a claim that there has been a worldwide conspiracy to hide the anti-COVID-19 benefits of Ivermectin.
Ivermectin is an anti-parasitic drug that was approved for use in humans in 1987. Over 3.4 billion doses have been given to humans since that time. Ivermectin also has well established antiviral and anti-inflammatory properties; thus early in the pandemic numerous doctors, desperate for solutions for their dying COVID-19 patients and with no other options, experimented with repurposing Ivermectin for their covid patients.
The US FDA , NIH and CDC advise against the use of Ivermectin for Covid-19.


In an excellent UnHerd article, Dr. Vinay Prasad MD, an Associate Professor of Epidemiology and Biostatistics at the UCSF, refutes a number of Dr. Malone’s more baseless claims while acknowledging others. Just as importantly, Dr. Prasad asserts that censorship of truthful information and scientific discussions regarding Covid-19 has been a real problem and source of the lack of faith in governmental health institutions and initiatives (i.e. conspiracy theories). Regarding the efficacy of ivermectin Dr. Prasad observes
“And Ivermectin has not shown persuasive evidence of benefit in randomized trials to date.’’
Given that the pandemic has been going on for 2+ years, and that during that time millions have received repurposed Ivermectin for its purported anti-Covid-19 properties, and that dozens of studies on its efficacy against Covid-19 have been published, it’s surprising that Dr. Prasad is not more definitive one way or the other. Thus, this issue seemed perfect for a Pure Science Substack article.
The Front Line Covid-19 Critical Care Consortium (FLCCC), a group of critical care physicians involved in the development of Covid-19 treatment protocols, is one of the largest proponents of Ivermectin use against Covid-19. They claim that prophylactic use and early treatment of Ivermectin can reduce Covid-19 deaths 40% to 75%!
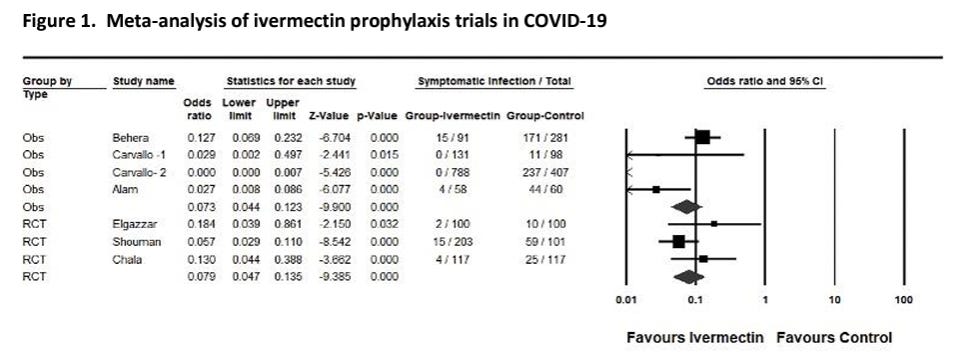
Critics attack the credibility of FLCCC evidence and claim most of their evidence lacks randomized clinical trials (RCTs), which should eliminate researcher bias (when conducted properly). RCTs are the gold standard for determining the efficacy of medical treatments. Dozens of published RCTs on use of Ivermectin paint a conflicting picture, in part because of widely varying treatment protocols and trial endpoints (definitions of success).
In June of 2021 a paper was published that collected the data from 15 RCT Ivermectin studies meeting their criteria and combined results in what's called a meta-analysis. The authors found:
“Moderate-certainty evidence finds that large reductions in COVID-19 deaths are possible using ivermectin. ’’
However, that paper and another similar meta-analysis of Ivermectin, were soon retracted when it was discovered that several of the component studies used in their analysis had fraudulent data.
Given the back and forth in claims regarding the efficacy of Ivermectin, along with evidence of fraudulent papers, it's understandable that reputable doctors are hesitant to be associated with Ivermectin. Also, now that better medicines are available in Developed Nations to both reduce susceptibility to Covid-19 (vaccines) and treat Covid-19 ( Paxlovid, molnupiravir, Remdesivir, Dexamethasone, etc.), some might argue that determining the efficacy of Ivermectin is a somewhat moot point. However from a global perspective it is not. As of January 30th 2022, worldwide covid-19 deaths stand at 5.66 million and growing at almost 8,000 a day, many of those in the Third World, where Ivermectin is cheap and ubiquitous but the majority of citizens have NO access to the advanced medicines listed above, and for billions still NO vaccines!
So what is the current best estimate of the effectiveness of Ivermectin to treat covid19? A more recent meta-analysis, which excludes the two component studies with evidence of fraud, concludes :
Ivermectin did not show a statistically significant effect on survival (RR, 0.90; 95% CI, 0.57 to 1.42; P = .66) (Figure 1I) or hospitalizations (RR, 0.63; 95% CI, 0.36 to 1.11; P = .11)
So does that mean Ivermectin doesn’t work? No! Let me deGeek that for you:
The studies show Ivermectin use improves survival and reduces hospitalizations, but we just don't have enough data to say so conclusively (with 95% confidence).
Here's the actual Forest Plot from that paper :
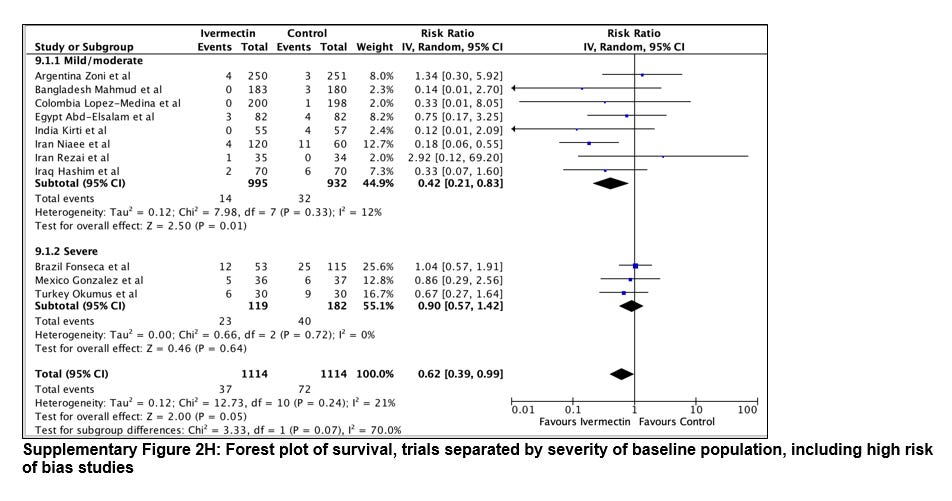
What this shows regarding surviving Covid-19:
Severe Covid-19 cases - Ivermectin has negligible benefit
Mild/moderate Covid cases - Ivermectin patients have average risk ratio of 0.42 (confidence range 0.21 to 0.83) - i.e. 58% fewer deaths with Ivermectin!
It’s tempting to stop here and conclude that the suppression of Ivermectin for early Covid-19 treatment has been a crime against humanity! I personally will wait until the TOGETHER clinical trial group publishes their results from a very large and very high quality study that concluded that Ivermectin DID NOT WORK (defined by minimum 37.5% relative risk reduction). I strongly suspect the paper will show Ivermectin reduced hospitalizations (the study primary endpoint) just not as much as their target.
What we can say now is that the preponderance of evidence is that Ivermectin has, at a minimum, a benefit based on mortality. So the answer to the title question of How Many Covid Deaths Would Ivermectin Have Saved?:
We can’t be sure, but the best evidence we have suggests that universal (with exclusions when contradicted for certain health conditions) Ivermectin treatment of all mild covid-19 cases, along with universal prophylaxis treatment of high risk groups like doctors and nurses would have saved between 430,000 (17%) and 2,000,000 (79%) Covid-19 deaths of the approximately 2.5 million deaths outside of Europe and the US (where competing and better treatments complicate analysis)